Quantifying the Effect of Supplementation with Algae and Its Extracts on Glycolipid Metabolism: A Meta-Analysis of Randomized Controlled Trials

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment and Publication Bias
2.5. Statistical Methods
3. Results
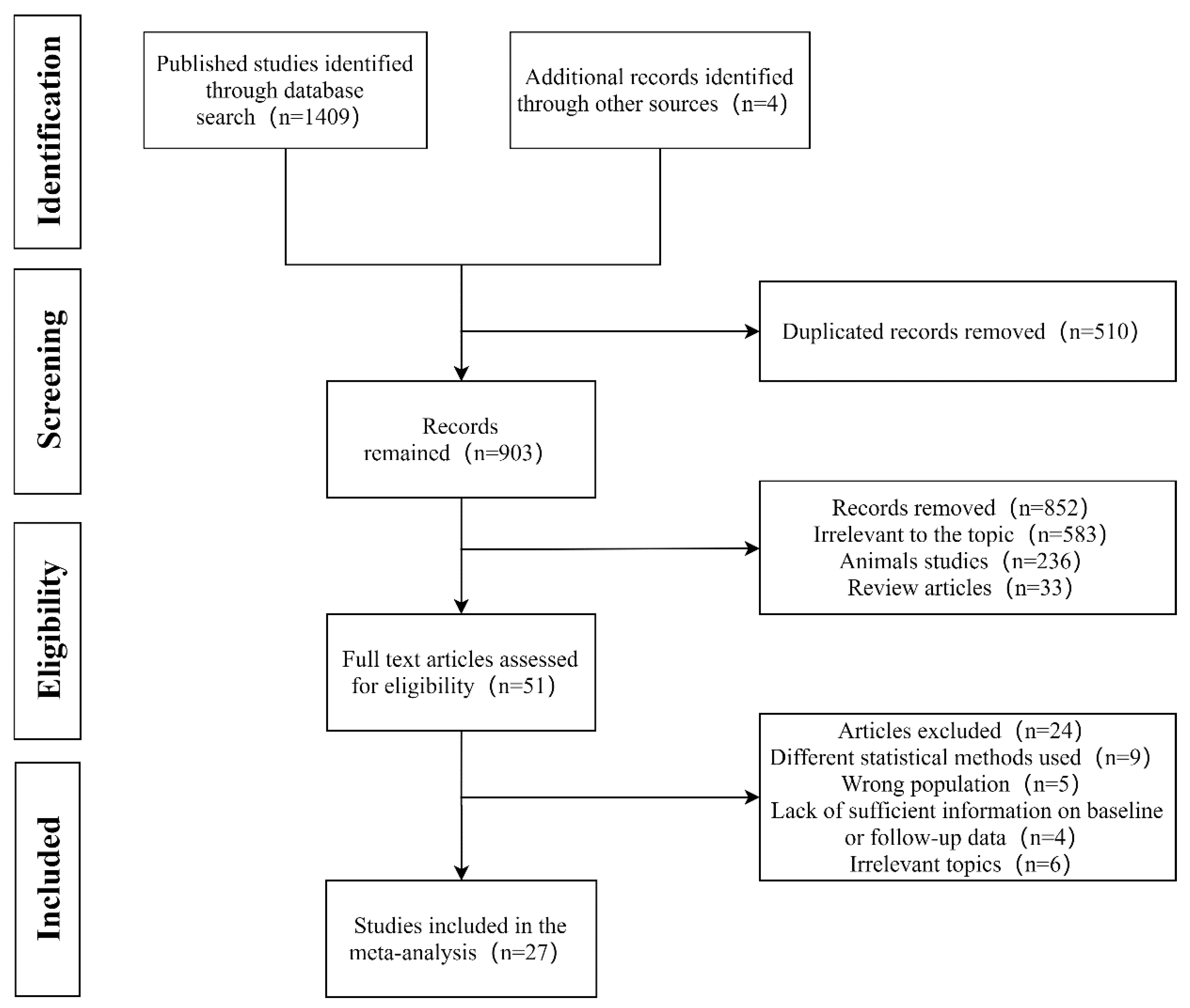
3.1. Search Results and Characteristics of Studies
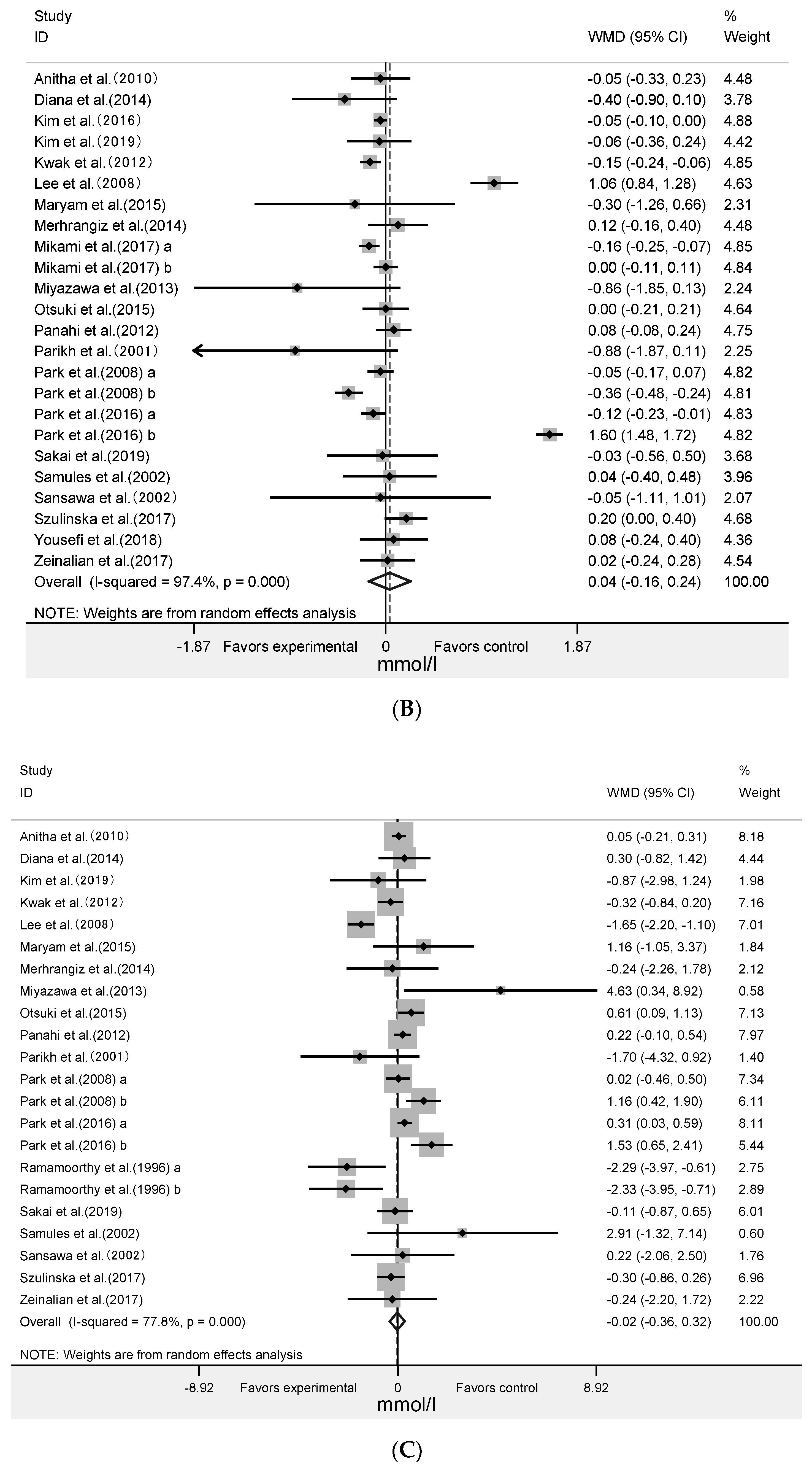
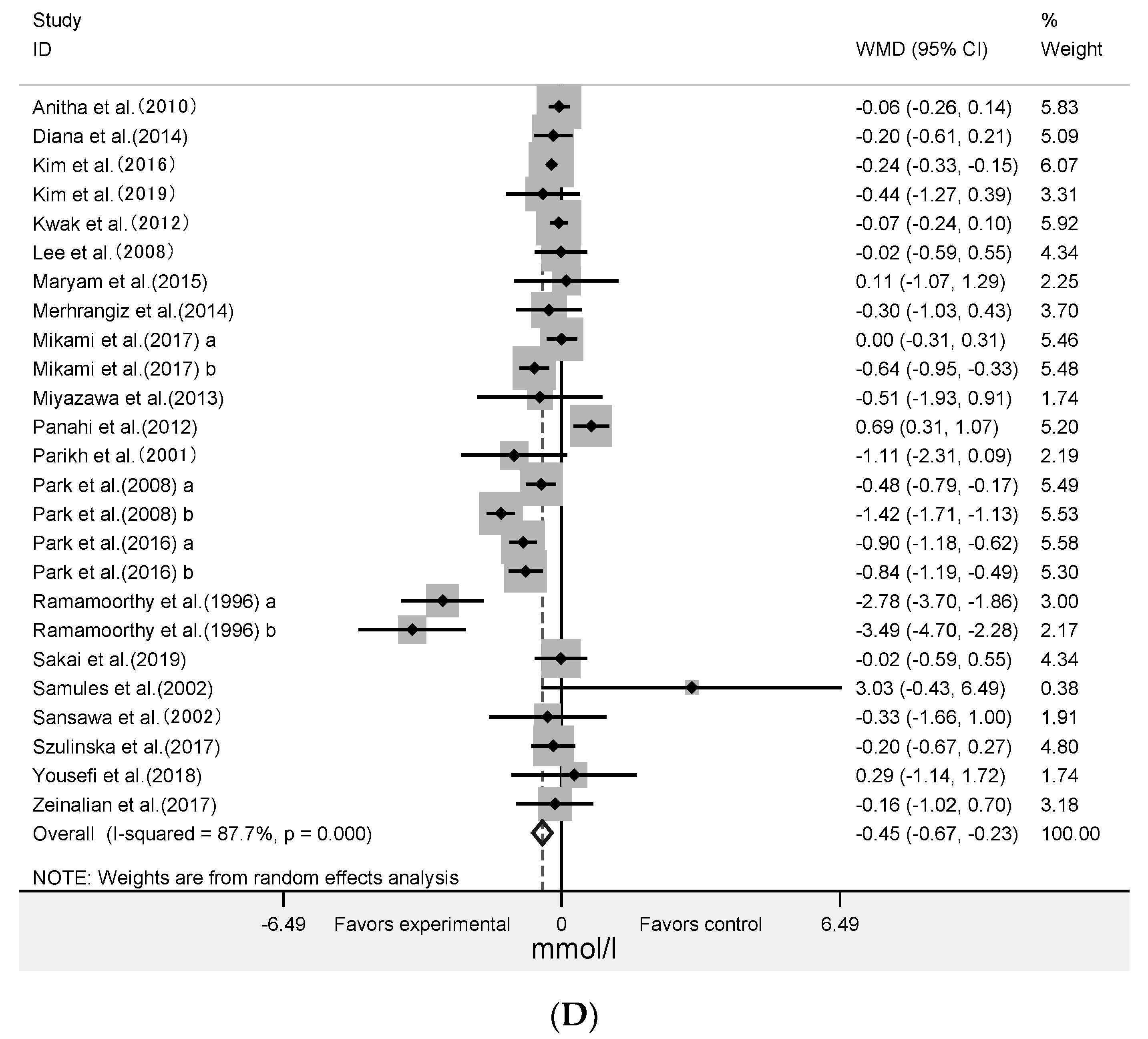
3.2. Effect of Algae and Its Extracts Intervention on Lipid Profiles
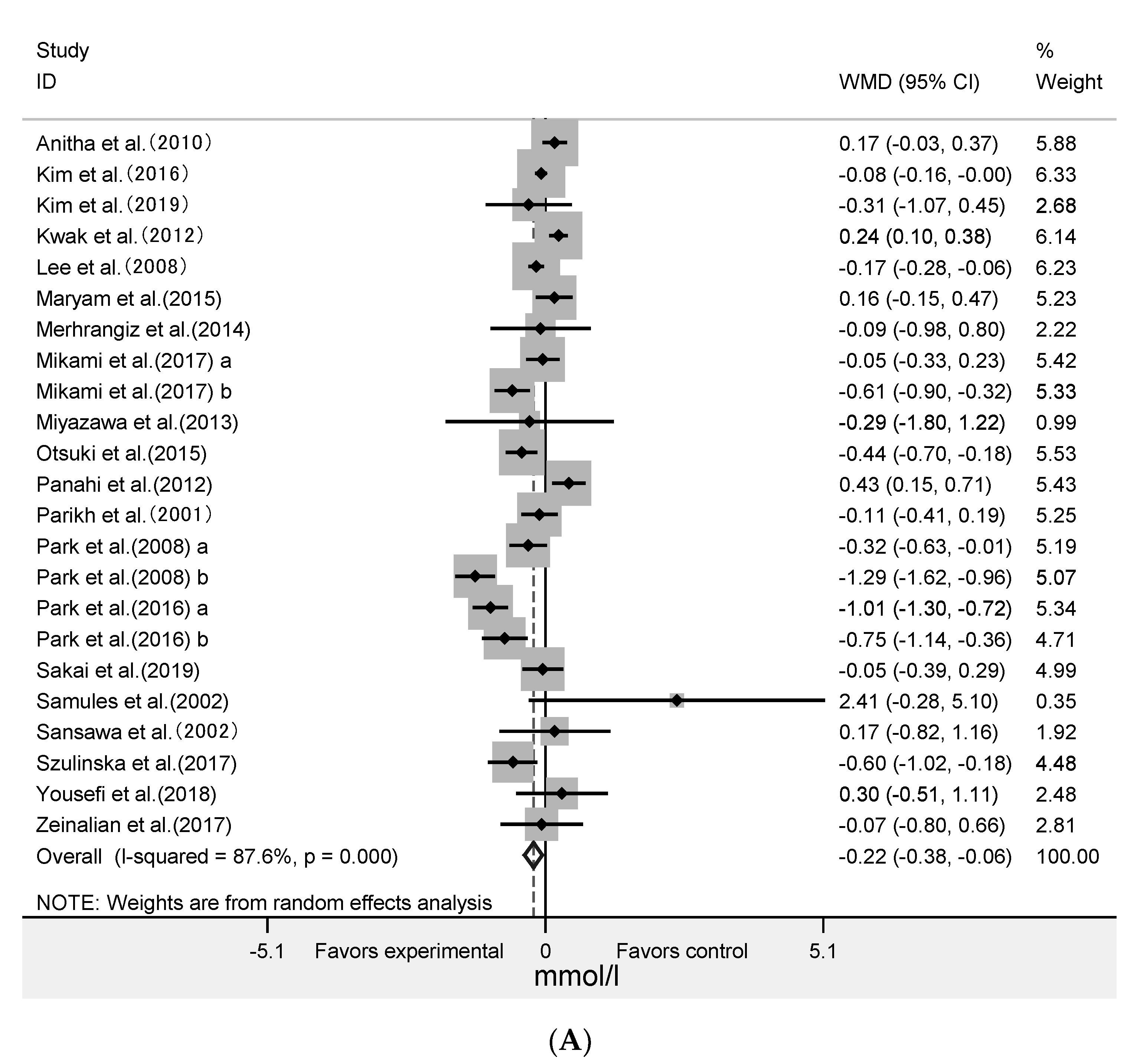
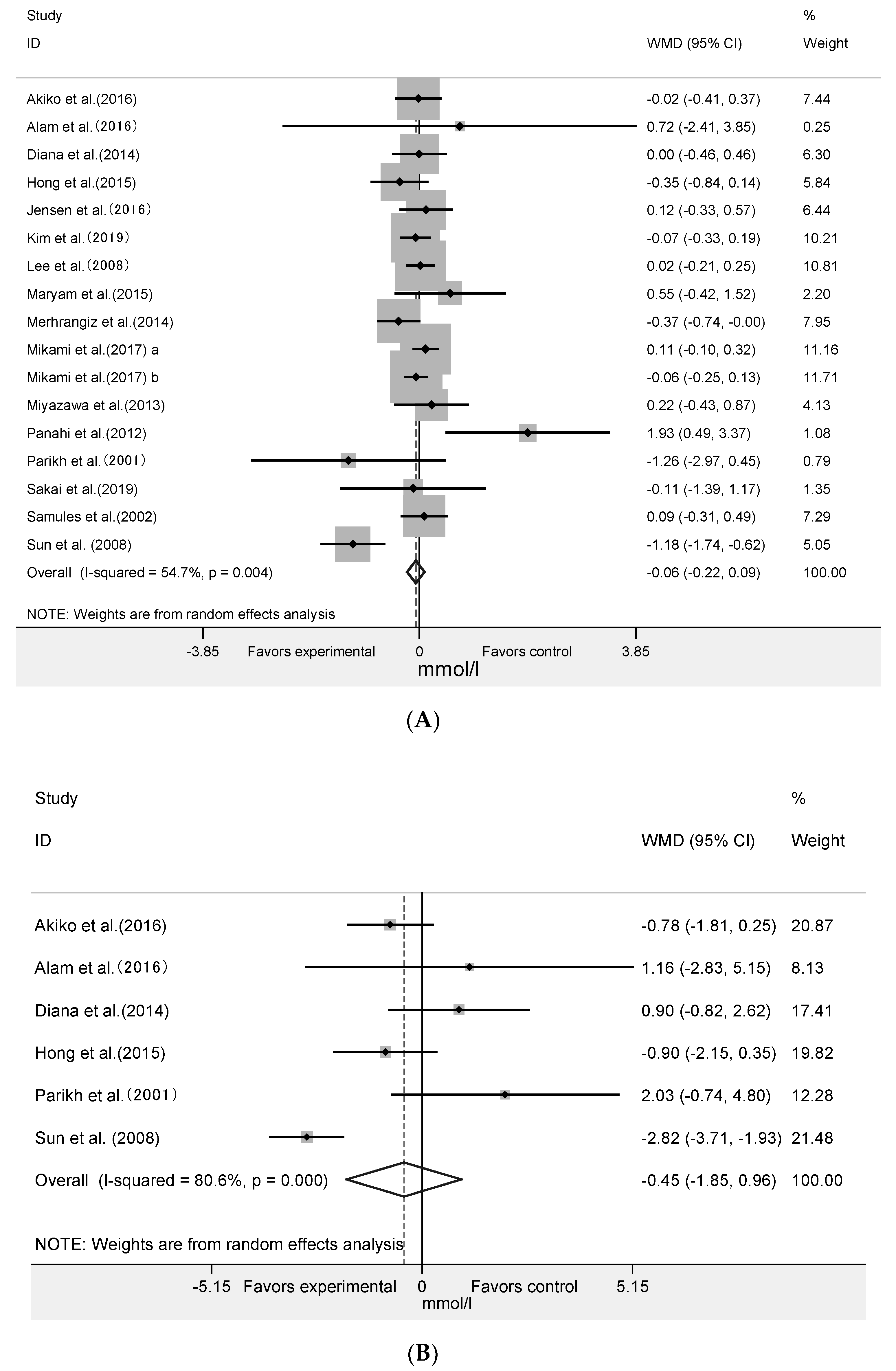
3.3. Effect of Algae and Its Extract Intervention on Fast Plasma Glucose and 2-Hour Postprandial Blood Glucose
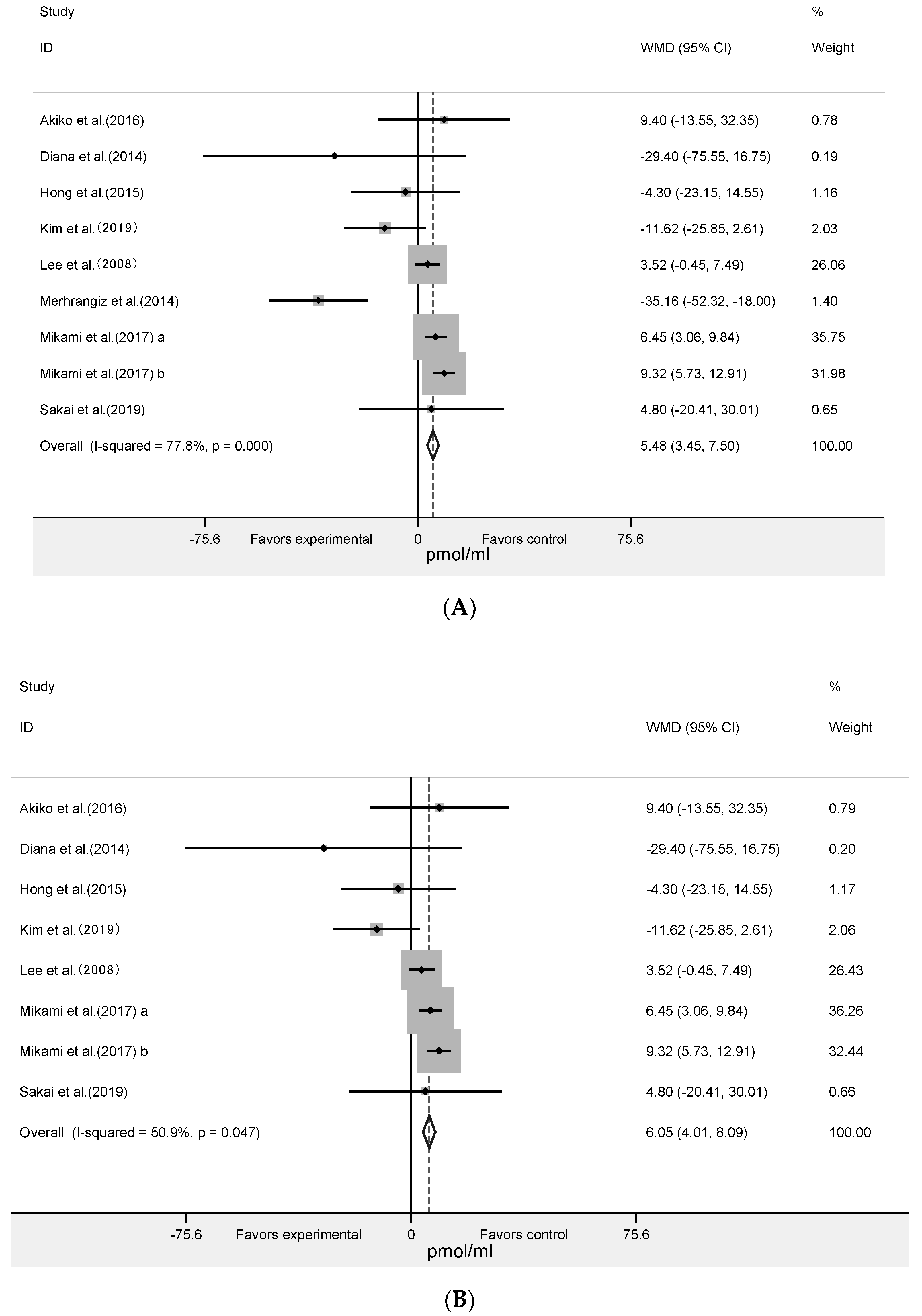
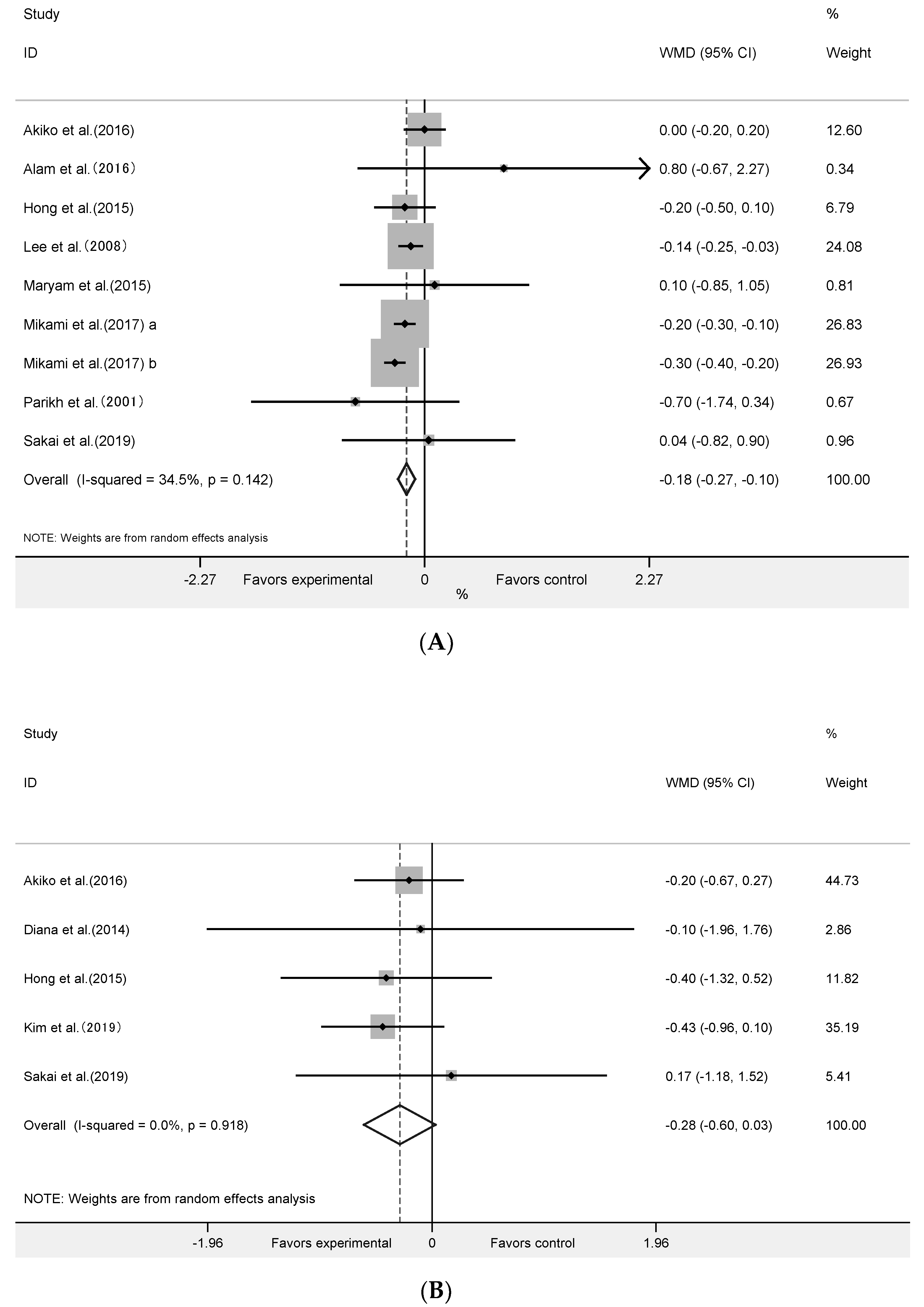
3.4. Effect of Algae and Its Extracts Intervention on HOMA-IR, Insulin and HbA1c
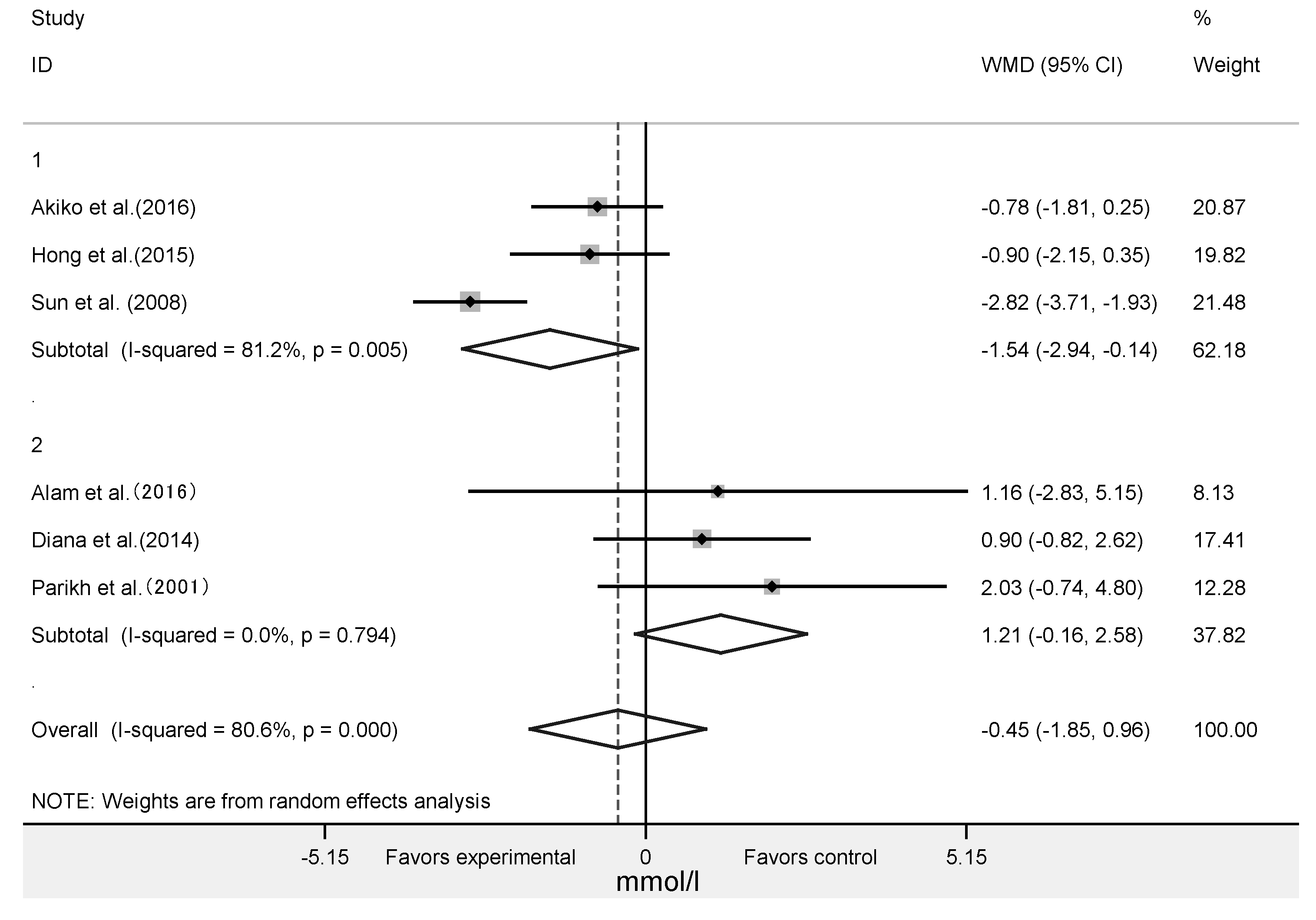
3.5. Subgroup Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| FPG | fasting plasma glucose |
| NA | not applicable |
| TG | triglycerides |
| TC | total cholesterol |
| HbA1c | glycosylated hemoglobin |
| FPG | fasting plasma glucose |
| 2hPBG | 2-h post-meal blood glucose |
| LDL-C | low-density lipoprotein cholesterol |
| HDL-C | high-density lipoprotein cholesterol |
| HOMA-IR | homeostasis model assessment-insulin resistance index |
References
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [Green Version]
- Cameron, A.; E Shaw, J.; Zimmet, P.Z. The metabolic syndrome: Prevalence in worldwide populations. Endocrinol. Metab. Clin. N. Am. 2004, 33, 351–375. [Google Scholar] [CrossRef]
- Smith, S.C.; Collins, A.; Ferrari, R.; Holmes, D.R.; Logstrup, S.; McGhie, D.V.; Ralston, J.; Sacco, R.L.; Stam, H.; Taubert, K.; et al. Our Time: A Call to Save Preventable Death from Cardiovascular Disease (Heart Disease and Stroke). J. Am. Coll. Cardiol. 2012, 60, 2343–2348. [Google Scholar] [CrossRef] [Green Version]
- Aviram, M. Atherosclerosis: Cell biology and lipoproteins–Inflammation and oxidative stress in atherogenesis: Protective role for paraoxonases. Curr. Opin. Lipidol. 2011, 22, 243–244. [Google Scholar] [CrossRef]
- Scannapieco, F.; Bush, R.B.; Paju, S. Associations between Periodontal Disease and Risk for Atherosclerosis, Cardiovascular Disease, and Stroke. A Systematic Review. Ann. Periodontol. 2003, 8, 38–53. [Google Scholar] [CrossRef]
- Drash, A. Atherosclerosis, cholesterol, and the pediatrician. J. Pediatr. 1972, 80, 693–696. [Google Scholar] [CrossRef]
- Kumagai, H.; Sakurai, M.; Takita, T.; Maruyama, Y.; Uno, S.; Ikegaya, N.; Kato, A.; Hishida, A. Association of Homocysteine and Asymmetric Dimethylarginine With Atherosclerosis and Cardiovascular Events in Maintenance Hemodialysis Patients. Am. J. Kidney Dis. 2006, 48, 797–805. [Google Scholar] [CrossRef]
- Neimann, A.L.; Shin, D.B.; Wang, X.; Margolis, D.J.; Troxel, A.; Gelfand, J.M. Prevalence of cardiovascular risk factors in patients with psoriasis. J. Am. Acad. Dermatol. 2006, 55, 829–835. [Google Scholar] [CrossRef]
- Haffner, S.M. Coronary Heart Disease in Patients with Diabetes. N. Engl. J. Med. 2000, 342, 1040–1042. [Google Scholar] [CrossRef]
- Shim, U.; Lee, H.; Oh, J.-Y.; Sung, Y.-A. Sleep Disorder and Cardiovascular Risk Factors among Patients with Type 2 Diabetes Mellitus. Korean J. Intern. Med. 2011, 26, 277–284. [Google Scholar] [CrossRef]
- Cho, N.; Shaw, J.E.; Karuranga, S.; Huang, Y.; Fernandes, J.D.D.R.; Ohlrogge, A.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Abdul, Q.A.; Choi, R.J.; Jung, H.A.; Choi, J.S. Health benefit of fucosterol from marine algae: A review. J. Sci. Food Agric. 2016, 96, 1856–1866. [Google Scholar] [CrossRef]
- Montero, L.; Sánchez-Camargo, A.D.P.; Ibáñez, E.; Gilbert-López, B.; Ibáñez, E. Phenolic Compounds from Edible Algae: Bioactivity and Health Benefits. Curr. Med. Chem. 2019, 25, 4808–4826. [Google Scholar] [CrossRef]
- Catarino, M.D.; Silva, A.; Cardoso, S.M. Phycochemical Constituents and Biological Activities of Fucus spp. Marine Drugs 2018, 16, 249. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, L.E.; Jeppesen, P.B.; Christiansen, C.B.; Hermansen, K.; Gregersen, S. Nordic Seaweed and Diabetes Prevention: Exploratory Studies in KK-Ay Mice. Nutrition 2019, 11, 1435. [Google Scholar] [CrossRef] [Green Version]
- Iso, H. Lifestyle and Cardiovascular Disease in Japan. J. Atheroscler. Thromb. 2011, 18, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Shin, A.; Lee, J.-S.; Youn, S.; Yoo, K.-Y. Dietary Factors and Breast Cancer in Korea: An Ecological Study. Breast J. 2009, 15, 683–686. [Google Scholar] [CrossRef]
- Deng, R.; Chow, T.-J. Hypolipidemic, Antioxidant, and Antiinflammatory Activities of Microalgae Spirulina. Cardiovasc. Ther. 2010, 28, e33–e45. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Galero, E.; Pérez-Pastén-Borja, R.; Perez-Juarez, A.; Favila-Castillo, L.; Gutiérrez-Salmeán, G.; Chamorro, G. Preclinical antitoxic properties of Spirulina (Arthrospira). Pharm. Biol. 2015, 54, 1–9. [Google Scholar] [CrossRef]
- Karkos, P.D.; Leong, S.C.; Karkos, C.D.; Sivaji, N.; Assimakopoulos, D.A. Spirulina in Clinical Practice: Evidence-Based Human Applications. Evid. Based Complement. Altern. Med. 2010, 2011, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Lu, Y.A.; Li, X.; Hyun, J.-M.; Kim, H.-S.; Lee, J.J.; Kim, T.H.; Kim, H.M.; Kang, M.-C.; Jeon, Y.-J.; et al. Anti-Obesity Effects of Grateloupia elliptica, a Red Seaweed, in Mice with High-Fat Diet-Induced Obesity via Suppression of Adipogenic Factors in White Adipose Tissue and Increased Thermogenic Factors in Brown Adipose Tissue. Nutrition 2020, 12, 308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, H.C.; Kim, S.H.; Park, Y.; Lee, B.H.; Hwang, H.J. Effects of 12-week Oral Supplementation of Ecklonia cava Polyphenols on Anthropometric and Blood Lipid Parameters in Overweight Korean Individuals: A Double-blind Randomized Clinical Trial. Phytother. Res. 2012, 26, 363–368. [Google Scholar] [CrossRef]
- Brown, E.; Allsopp, P.J.; Magee, P.J.; Gill, C.I.; Nitecki, S.; Strain, C.R.; McSorley, E.M. Seaweed and human health. Nutr. Rev. 2014, 72, 205–216. [Google Scholar] [CrossRef]
- Taichi, S.; Shinichi, K.; Atsushi, H.; Kaori, O.; Yuki, S.; Naoki, N.; Yoshikazu, N.; Yoshitaka, T.; Ichiro, T. Dietary patterns and cardiovascular disease mortality in Japan: A prospective cohort study. Int. J. Epidemiol. 2007, 3, 600–609. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.Y.; Won, J.C.; Kang, Y.J.; Yoon, S.H.; Choi, E.-O.; Bae, J.Y.; Sung, M.H.; Kim, H.-R.; Yang, J.H.; Oh, J.; et al. Type 2 Diabetes in Urban and Rural Districts in Korea: Factors Associated with Prevalence Difference. J. Korean Med. Sci. 2010, 25, 1777–1783. [Google Scholar] [CrossRef]
- Shin, A.; Lim, S.-Y.; Sung, J.; Shin, H.-R.; Kim, J. Dietary Intake, Eating Habits, and Metabolic Syndrome in Korean Men. J. Am. Diet. Assoc. 2009, 109, 633–640. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R.L. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biomedical 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Sakai, C.; Abe, S.; Kouzuki, M.; Shimohiro, H.; Ota, Y.; Sakinada, H.; Takeuchi, T.; Okura, T.; Kasagi, T.; Hanaki, K. A Randomized Placebo-controlled Trial of an Oral Preparation of High Molecular Weight Fucoidan in Patients with Type 2 Diabetes with Evaluation of Taste Sensitivity. Yonago Acta Med. 2019, 62, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Sanaei, M.; Ebrahimi, M.; Banazadeh, Z.; Shafiee, G.; Khatami, F.; Ahadi, Z.; Heshmat, R. Consequences of AphanizomenonFlos-aqua e( AFA ) extract ( Stemtech TM ) on metabolic profile of patients with type 2 diabetes. J. Diabetes Metab. Disord. 2015, 14, 50. [Google Scholar] [CrossRef] [Green Version]
- Sun, K.M.; Yun, K.J.; Hwan, C.W.; Sun, L.S. Effects of seaweed supplementation on blood glucose concentration, lipid profile, and antioxidant enzyme activities in patients with type 2 diabetes mellitus. Nutri. Res. Pract. 2008, 2, 62–67. [Google Scholar]
- Lee, S.H.; Jeon, Y.J. Efficacy and safety of a dieckol-rich extract (AG-dieckol) of brown algae, Ecklonia cava, in pre-diabetic individuals: A double-blind, randomized, placebo-controlled clinical trial. Food Funct. 2015, 6, 853–858. [Google Scholar] [CrossRef]
- Alam, A.; Quamri, S.; Fatima, S.; Roqaiya, M.; Ahmad, Z. Efficacy of Spirulina (Tahlab) in Patients of Type 2 Diabetes Mellitus (Ziabetus Shakri)—A Randomized Controlled Trial. J. Diabetes Metab. 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.H.; Park, J.-E.; Choi, Y.-J.; Huh, K.-B.; Kim, W.Y. A randomized study to establish the effects of spirulina in type 2 diabetes mellitus patients. Nutr. Res. Pract. 2008, 2, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Parikh, P.; Mani, U.; Iyer, U. Role of Spirulina in the Control of Glycemia and Lipidemia in Type 2 Diabetes Mellitus. J. Med. Food 2001, 4, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Anitha, L.; Chandralekha, K. Effect of supplementation of Spirulina on blood glucose, glycosylated hemoglobin and lipid profile of male noninsulin dependent diabetics. Asian J. Exp. Biol. Sci. 2010, 1, 36–46. [Google Scholar]
- Sansawa, H.; Inoue, K.; Shirai, T. Effect of Chlorella Tablet Ingestion on Mild Hypercholesterolemic Patients. Nippon. Shokuhin Kagaku Kogaku Kaishi 2002, 49, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Mikami, N.; Hosokawa, M.; Miyashita, K.; Sohma, H.; Ito, Y.M.; Kokai, Y. Reduction of HbA1c levels by fucoxanthin-enriched akamoku oil possibly involves the thrifty allele of uncoupling protein 1 (UCP1): A randomised controlled trial in normal-weight and obese Japanese adults. J. Nutr. Sci. 2017, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Park, H.-J.; Lee, H.S. The influence of obesity on the effects of spirulina supplementation in the human metabolic response of Korean elderly. Nutr. Res. Pract. 2016, 10, 418–423. [Google Scholar] [CrossRef]
- Kim, C.O.; Kim, Y.N.; Lee, D.-C. Effects of Gelidium elegans on Weight and Fat Mass Reduction and Obesity Biomarkers in Overweight or Obese Adults: A Randomized Double-Blinded Study. Nutrition 2019, 11, 1513. [Google Scholar] [CrossRef] [Green Version]
- Yousefi, R.; Mottaghi, A.; Saidpour, A. Spirulina platensis effectively ameliorates anthropometric measurements and obesity-related metabolic disorders in obese or overweight healthy individuals: A randomized controlled trial. Complement. Ther. Med. 2018, 40, 106–112. [Google Scholar] [CrossRef]
- Ebrahimi-Mameghani, M.; Aliashrafi, S.; Javadzadeh, Y.; AsghariJafarabadi, M. The Effect of Chlorella vulgaris Supplementation on Liver Enzymes, Serum Glucose and Lipid Profile in Patients with Non-Alcoholic Fatty Liver Disease. Health Promot. Perspect. 2014, 4, 107–115. [Google Scholar]
- Panahi, Y.; Pishgoo, B.; Jalalian, H.; Mohammadi, E.; Taghipour, H.R.; Sahebkar, A.; Abolhasani, E. Investigation of the effects of Chlorella vulgaris as an adjunctive therapy for dyslipidemia: Results of a randomised open-label clinical trial. Nutr. Diet. 2012, 69, 13–19. [Google Scholar] [CrossRef]
- Takeshi, O.; Kazuhiro, S.; Seiji, M. Changes in arterial stiffness and nitric oxide production with Chlorella-derived multicomponent supplementation in middle-aged and older individuals. J. Clin. Biochem. Nutr. 2015, 57, 228–232. [Google Scholar]
- Taiki, M.; Kiyotaka, N.; Hideo, T.; Ohki, H.; Shunji, K.; Momoko, K.; Fumiko, K.; Teruo, M. Ingestion of Chlorella Reduced the Oxidation of Erythrocyte Membrane Lipids in Senior Japanese Subjects. J. Oleo Sci. 2013, 62, 873–881. [Google Scholar]
- Kwak, J.H.; Baek, S.H.; Woo, Y.; Han, J.K.; Kim, B.G.; Kim, O.Y.; Lee, J.H. Beneficial immunostimulatory effect of short-termChlorellasupplementation: Enhancement ofNatural Killercell activity and early inflammatory response (Randomized, double-blinded, placebo-controlled trial). Nutr. J. 2012, 11, 53. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, J.; Lim, Y.; Kim, Y.J.; Kim, J.Y.; Kwon, O. A dietary cholesterol challenge study to assess Chlorella supplementation in maintaining healthy lipid levels in adults: A double-blinded, randomized, placebo-Controlled study. Nutr. J. 2016, 15, 54. [Google Scholar] [CrossRef] [Green Version]
- Szulinska, M.; Gibas-Dorna, M.; Miller-Kasprzak, E.; Suliburska, J.; Miczke, A.; Walczak-Gałezewska, M.; Stelmach-Mardas, M.; Walkowiak, J.; Bogdanski, P. Spirulina maxima improves insulin sensitivity, lipid profile, and total antioxidant status in obese patients with well-treated hypertension: A randomized double-blind placebo-Controlled study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2473–2481. [Google Scholar]
- Zeinalian, R.; Farhangi, M.A.; Shariat, A.; Saghafi-Asl, M. The effects of Spirulina Platensis on anthropometric indices, appetite, lipid profile and serum vascular endothelial growth factor (VEGF) in obese individuals: A randomized double blinded placebo controlled trial. BMC Complement. Altern. Med. 2017, 17, 225. [Google Scholar] [CrossRef]
- Samuels, R.; Mani, U.V.; Iyer, U.M.; Nayak, U.S. Hypocholesterolemic Effect of Spirulina in Patients with Hyperlipidemic Nephrotic Syndrome. J. Med. Food 2002, 5, 91–96. [Google Scholar] [CrossRef]
- Ramamoorthy, A.; Premakumari, S. Effect of supplementation of spirulina on Hypercholesterolemic patients. J. Food Sci. Technol. 1996, 33, 124–128. [Google Scholar]
- Park, H.J.; Lee, Y.J.; Ryu, H.K.; Kim, M.-H.; Chung, H.W.; Kim, W.Y. A Randomized Double-Blind, Placebo-Controlled Study to Establish the Effects of Spirulina in Elderly Koreans. Ann. Nutr. Metab. 2008, 52, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.S.; Drapeau, C.; Lenninger, M.; Benson, K.F. Clinical Safety of a High Dose of Phycocyanin-Enriched Aqueous Extract from Arthrospira (Spirulina) platensis: Results from a Randomized, Double-Blind, Placebo-Controlled Study with a Focus on Anticoagulant Activity and Platelet Activation. J. Med. Food 2016, 19, 645–653. [Google Scholar] [CrossRef] [Green Version]
- Corona, D.M.H.; Martínez-Abundis, E.; González-Ortiz, M. Effect of Fucoidan Administration on Insulin Secretion and Insulin Resistance in Overweight or Obese Adults. J. Med. Food 2014, 17, 830–832. [Google Scholar] [CrossRef]
- Mizote, A.; Yamada, M.; Yoshizane, C.; Arai, N.; Maruta, K.; Arai, S.; Endo, S.; Ogawa, R.; Mitsuzumi, H.; Ariyasu, T.; et al. Daily Intake of Trehalose Is Effective in the Prevention of Lifestyle-Related Diseases in Individuals with Risk Factors for Metabolic Syndrome. J. Nutr. Sci. Vitaminol. 2016, 62, 380–387. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Liao, D.; Pu, R.; Cui, Y. Quantifying the effects of spirulina supplementation on plasma lipid and glucose concentrations, body weight, and blood pressure. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 729–742. [Google Scholar] [CrossRef] [Green Version]
- Serban, M.-C.; Sahebkar, A.; Dragan, S.; Andrica, F.; Urosniu, S.; Banach, M. A systematic review and meta-analysis of the impact of spirulina supplementation on plasma lipid concentrations. Atherosclerosis 2015, 241, e191. [Google Scholar] [CrossRef]
- Marathe, P.H.; Gao, H.X.; Close, K.L. American Diabetes Association Standards of Medical Care in Diabetes 2017. J. Diabetes 2017, 9, 320–324. [Google Scholar] [CrossRef]
- Hammoud, T.; Tanguay, J.-F.; Bourassa, M.G. Management of coronary artery disease: Therapeutic options in patients with diabetes. J. Am. Coll. Cardiol. 2000, 36, 355–365. [Google Scholar] [CrossRef] [Green Version]
- Shafrir, E. Development and consequences of insulin resistance: Lessons from animals with hyperinsulinaemia. Diabetes Metab. 1996, 22, 122–131. [Google Scholar]
- Schröder, H. Protective mechanisms of the Mediterranean diet in obesity and type 2 diabetes. J. Nutr. Biochem. 2007, 18, 149–160. [Google Scholar] [CrossRef]
- Murata, M.; Ishihara, K.; Saito, H. Hepatic fatty acid oxidation enzyme activities are stimulated in rats fed the brown seaweed, Undaria pinnatifida (wakame). J. Nutr. 1999, 129, 146–151. [Google Scholar] [CrossRef]
- Maeda, H.; Hosokawa, M.; Sashima, T.; Murakami-Funayama, K.; Miyashita, K. Anti-obesity and anti-diabetic effects of fucoxanthin on diet-induced obesity conditions in a murine model. Mol. Med. Rep. 2009, 2, 897–902. [Google Scholar] [CrossRef]
- Nagaoka, S.; Shimizu, K.; Kaneko, H.; Shibayama, F.; Morikawa, K.; Kanamaru, Y.; Otsuka, A.; Hirahashi, T.; Kato, T. A Novel Protein C-Phycocyanin Plays a Crucial Role in the Hypocholesterolemic Action of Spirulina platensis Concentrate in Rats. J. Nutr. 2005, 135, 2425–2430. [Google Scholar] [CrossRef] [Green Version]
- Kulshreshtha, A.; Jarouliya, U.; Bhadauriya, P.; Prasad, G.; Bisen, P. Spirulina in Health Care Management. Curr. Pharm. Biotechnol. 2008, 9, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Upasani, C.D.; Balaraman, R. Protective effect of Spirulina on lead induced deleterious changes in the lipid peroxidation and endogenous antioxidants in rats. Phytother. Res. 2003, 17, 330–334. [Google Scholar] [CrossRef]
- Miczke, A.; Szulińska, M.; Hansdorfer-Korzon, R.; Kręgielska-Narożna, M.; Suliburska, J.; Walkowiak, J.; Skrypnik, D. Effects of spirulina consumption on body weight, blood pressure, and endothelial function in overweight hypertensive Caucasians: A double-blind, placebo-controlled, randomized trial. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 150–156. [Google Scholar]
- Ku, C.S.; Yang, Y.; Park, Y.; Lee, J. Health Benefits of Blue-Green Algae: Prevention of Cardiovascular Disease and Nonalcoholic Fatty Liver Disease. J. Med. Food 2013, 16, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Turner, R.C.; Millns, H.; Neil, H.A.W.; Stratton, I.; E Manley, S.; Matthews, D.R.; Holman, R.R. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom prospective diabetes study (UKPDS: 23). BMJ 1998, 316, 823–828. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S.; Mokdad, A.H. Fruit and Vegetable Consumption and Diabetes Mellitus Incidence among U.S. Adults. Prev. Med. 2001, 32, 33–39. [Google Scholar] [CrossRef]
- Qureshi, A.A.; Sami, S.A.; Khan, F.A. Effects of stabilized rice bran, its soluble and fiber fractions on blood glucose levels and serum lipid parameters in humans with diabetes mellitus Types I and II. J. Nutr. Biochem. 2002, 13, 175–187. [Google Scholar] [CrossRef]
- Jurkovic, N.; Kolb, N.; Colic, I. Nutritive value of marine algaeLaminaria japonica and Undaria pinnatifida. Food/Nahrung 1995, 39, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Urbano, M.G.; Goñi, I. Bioavailability of nutrients in rats fed on edible seaweeds, Nori (Porphyra tenera) and Wakame (Undaria pinnatifida), as a source of dietary fibre. Food Chem. 2002, 76, 281–286. [Google Scholar] [CrossRef]
- Lahaye, M. Marine algae as sources of fibres: Determination of soluble and insoluble dietary fibre contents in some ‘sea vegetables’. J. Sci. Food Agric. 1991, 54, 587–594. [Google Scholar] [CrossRef]
- Wong, K.H.; Sam, S.; Cheung, P.; Ang, P. Changes in lipid profiles of rats fed with seaweed-based diets. Nutr. Res. 1999, 19, 1519–1527. [Google Scholar] [CrossRef]
- Mani, U.V.; Desai, S.; Iyer, U. Studies on the Long-Term Effect of Spirulina Supplementation on Serum Lipid Profile and Glycated Proteins in NIDDM Patients. J. Nutraceuticals Funct. Med. Foods 2000, 2, 25–32. [Google Scholar] [CrossRef]
- A Westphal, S.; Gannon, M.C.; Nuttall, F.Q. Metabolic response to glucose ingested with various amounts of protein. Am. J. Clin. Nutr. 1990, 52, 267–272. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (year) | Country | RCT Design | Sample Number | Male (%) | Age (year) | Health Status | Intervention Duration | Intervention Products | Main Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Ramamoorthy et al. [51] (1996) | India | NA | 20 | NA | 40–60 | Hypercholesterolemia subjects | 3 months | Spirulina (2 g/day; 4 g/day) | TG, TC |
| Parikh et al. [35] (2001) | India | Parallel | 25 | 60% | 46–61 | patients with type 2 diabetes | 2 months | Spirulina tablets (1 g/day) | HbA1c, FPG, 2hPBG, LDL–C, HDL–C, TG, TC |
| Samules et al. [50] (2002) | India | Parallel | 23 | 74% | 3–12 | patients with hyperlipidemic nephrotic syndrome | 2 months | Spray–dried spirulina capsules (3 g/day) | FPG, LDL–C, HDL–C, TG, TC |
| Sansawa et al. [37] (2002) | Japan | NA | 20 | 40% | 45–64 | Hyperlipidemia subjects | 3 months | Chlorella (3 g/day) | LDL–C, HDL–C, TG, TC |
| Lee et al. [34] (2008) | Korea | Parallel | 37 | 54% | 49–56 | patients with type 2 diabetes | 12 weeks | Spirulina pills from freeze–dried spirulina (8 g/day) | HbA1c, FPG, Insulin LDL–C, HDL–C, TG, TC |
| Park et al. [52] (2008) | Korea | Parallel | 43; 36 | 100% | 64–68 | males aged 60–87; females aged 60–87 | 16 weeks | Freezedried spirulina pills (8 g/day) | LDL–C, HDL–C, TG, TC |
| Sun et al. [31] (2008) | Korea | NA | 20 | 45% | 51–58 | patients with type 2 diabetes | 4 weeks | Pills with sea tangle and sea mustard (48 g/day) | FPG, 2hPBG |
| Anitha et al. [36] (2010) | India | Parallel | 80 | 100% | 45–60 | patients with type 2 diabetes | 12 weeks | Spirulina capsules and diet modification (1 g/day) | LDL–C, HDL–C, TG, TC |
| Kwak et al. [46] (2012) | Korea | Parallel | 51 | 39% | 30–38 | healthy subjects | 8 weeks | Chlorella (5 g/day) | LDL–C, HDL–C, TG, TC |
| Panahi et al. [43] (2012) | Iran | NA | 63 | 27% | 51–73 | dyslipidemic subjects | 8 weeks | Chlorella and atorvastatin (0.6 g/day) | FPG, LDL–C, HDL–C, TG, TC |
| Miyazawa et al. [45] (2013) | Japan | Parallel | 12 | 58% | 50–65 | nomal senior subjects | 2 months | Chlorella (8 g/day) | FPG, LDL–C, HDL–C, TG, TC |
| Diana et al. [54] (2014) | Mexico | Parallel | 21 | 29% | 38–53 | overweight or obese adult | 3 months | Fucoidan (0.5 g/day) | FPG, 2hPBG, HOMA–IR, insulin, LDL–C, TG, TC |
| Merhrangiz et al. [42] (2014) | Iran | Parallel | 55 | 55% | 20–50 | obese patients with NAFLD | 8 weeks | Chlorella (1.2 g/day) | FPG, insulin, LDL–C, HDL–C, TG, TC |
| Hong et al. [32] (2015) | Korea | Cross–over | 73 | 71% | 45–62 | pre–diabetic adults | 12 weeks | Tablets with AG–dieckol (1.5 g/day) | HbA1c, FPG, 2hPBG, Insulin |
| Maryam et al. [30] (2015) | Iran | Parallel | 49 | 18% | 48–65 | patients with type 2 diabetes | 12 weeks | Capsules of Aogenizomenon extract (3 g/day) | HbA1c, FPG, LDL–C, HDL–C, TG, TC |
| Otsuki et al. [44] (2015) | Japan | Parallel | 32 | 41% | 45–75 | adult subjects | 4 weeks | Chlorella (6 g/day) | LDL–C, HDL–C, TG |
| Akiko et al. [55] (2016) | Japan | Parallel | 34 | 97% | 40–56 | healthy subjects, BMI ≥ 23 | 16 weeks | Trehalose (10 g/day) | FPG, 2hPBG, HOMA–IR, insulin, HbA1c |
| Alam et al. [33] (2016) | India | NA | 40 | NA | 35–54 | patients with type 2 diabetes | 45 days | Spirulina powder (14 g/day) | HbA1c, FPG, 2hPBG |
| Jensen et al. [53] (2016) | America | Parallel | 24 | 21% | 25–62 | adult men and women 25–65 years of age | 2 weeks | Phycocyaninenriched aqueous extract from Spirulina platensis (2.3 g/day) | FPG |
| Kim et al. [47] (2016) | Korea | Parallel | 34 | 12% | 22–25 | healthy subjects | 4 weeks | Chlorella (5 g/day) | LDL–C, HDL–C, TC |
| Park et al. [39] (2016) | Korea | Parallel | 45; 33 | NA | 64–69 | Non–obese subjects; obese subjects | 12 weeks | Spirulina (8 g/day) | LDL–C, HDL–C, TG, TC |
| Mikami et al. [38] (2017) | Japan | Parallel | 39; 40 | 67%; 73% | 50–60 | obese subjects, BMI ≥ 22 | 8 weeks | Fucoidan (1 g/day; 2g/day) | FPG, insulin, HbA1c, LDL–C, HDL–C, TC |
| Szulinska et al. [48] (2017) | Poland | Parallel | 50 | 50% | 40–58 | subjects with treated hypertension | 12 weeks | Spirulina capsules (2 g/day) | LDL–C, HDL–C, TG, TC |
| Zeinalian et al. [49] (2017) | Iran | Parallel | 56 | 16% | 25–43 | obese individuals | 12 weeks | Spirulina platensis supplement (1 g/day) | LDL–C, HDL–C, TG, TC |
| Yousefi et al. [41] (2018) | Iran | Parallel | 38 | 18% | 31–51 | obese and overweight subjects | 12 weeks | Spirulina (2 g/day) | LDL–C, HDL–C, TC |
| Kim et al. [40] (2019) | Korea | Parallel | 78 | 40% | 27–46 | obese or overweight individuals | 12 weeks | Gelidium elegans (1 g/day) | FPG, HOMA–IR, insulin, LDL–C, HDL–C, TG, TC |
| Sakai et al. [29] (2019) | Japan | Cross–over | 30 | 73% | 30–79 | patients with type 2 diabetes | 28 weeks | Fucoidan (1.62 g/day) | HbA1c, FPG, Insulin, LDL–C, HDL–C, TG, TC |
| Outcome | Variable | No. of Trials | Effect Size (95% CI) | p-Value | I2 (%) |
|---|---|---|---|---|---|
| FPG(mmol/L) | Intervention duration | ||||
| <10 weeks | 9 | −0.087 (−0.362, 0.189) | 0.538 | 71.9 | |
| >10 weeks | 6 | −0.034 (−0.173, 0.106) | 0.636 | 0.0 | |
| Sample size | |||||
| <40 | 9 | −0.064 (−0.279, 0.151) | 0.559 | 57.8 | |
| ≥40 | 6 | −0.073 (−0.327, 0.181) | 0.575 | 53.4 | |
| Intervention species | |||||
| Spirulina | 5 | 0.038 (−0.142, 0.218) | 0.680 | 0.0 | |
| Chlorella | 3 | 0.343 (−0.592, 1.279) | 0.472 | 81.1 | |
| Others | 9 | −0.121 (−0.327, 0.085) | 0.249 | 61.8 | |
| Health condition | |||||
| Health | 3 | 0.071 (−1.099, 0.342) | 0.604 | 0.0 | |
| Type 2 diabetes | 7 | −0.313 (−0.817, 0.191) | 0.223 | 69.7 | |
| Obesity | 5 | −0.047 (−0.181, 0.087) | 0.491 | 22.7 | |
| Other unhealth conditions | 2 | 0.874 (−0.909, 2.657) | 0.337 | 82.7 | |
| Area | |||||
| East Asia | 8 | −0.011 (−0.111, 0.090) | 0.833 | 0.0 | |
| Non−Asia | 2 | 0.061 (−0.263, 0.385) | 0.711 | 0.0 | |
| Southwest Asia | 7 | −0.098 (−0.710, 0.515) | 0.754 | 77.7 | |
| Insulin(pmol/mL) | Intervention duration | ||||
| <10 weeks | 3 | −0.636 (−11.138, 9.866) | 0.905 | 92.0 | |
| >10 weeks | 6 | −0.299 (−7.456, 6.858) | 0.935 | 25.7 | |
| Sample size | |||||
| <40 | 4 | −9.597 (29.892, 10.697) | 0.354 | 90.8 | |
| ≥40 | 5 | 5.157 (2.611, 7.703) | 0.000 * | 0.0 | |
| HDL−C(mmol/L) | Intervention duration | ||||
| <10 weeks | 10 | −0.068 (−0.276, 0.139) | 0.519 | 83.8 | |
| >10 weeks | 13 | −0.329 (−0.595, −0.064) | 0.015 * | 88.4 | |
| Sample size | |||||
| <40 | 11 | −0.158 (−0.441, 0.124) | 0.272 | 89.5 | |
| ≥40 | 12 | −0.298 (−0.507, −0.089) | 0.005 * | 84.9 | |
| Intervention species | |||||
| Spirulina | 11 | −0.382 (−0.683, −0.080) | 0.013 * | 89.9 | |
| Chlorella | 7 | 0.028 (−0.218, 0.274) | 0.821 | 83.6 | |
| Others | 5 | −0.158 (−0.455, 0.140) | 0.299 | 73.2 | |
| Health condition | |||||
| Health | 7 | −0.456 (−0.817, −0.094) | 0.013 * | 94.9 | |
| Type 2 diabetes | 5 | −0.010 (−0.181, 0.162) | 0.912 | 63.8 | |
| Obesity | 7 | −0.303 (−0.600, −0.006) | 0.046 * | 60.0 | |
| Other unhealth conditions | 4 | 0.158 (−0.626, 0.942) | 0.692 | 84.0 | |
| Area | |||||
| East Asia | 14 | −0.368 (−0.573, −0.163) | 0.000 * | 90.7 | |
| Non−Asia | 1 | − | − | − | |
| Southwest Asia | 8 | 0.164 (−0.009, 0.336) | 0.063 | 31.3 | |
| LDL−C(mmol/L) | Intervention duration | ||||
| <10 weeks | 10 | −0.059 (−0.129, 0.011) | 0.101 | 54.9 | |
| >10 weeks | 14 | 0.129 (−0.276, 0.533) | 0.533 | 98.3 | |
| Sample size | |||||
| <40 | 11 | 0.121 (−0.314, 0.557) | 0.585 | 98.8 | |
| ≥40 | 13 | −0.028 (−0.094, 0.039) | 0.418 | 42.7 | |
| Intervention species | |||||
| Spirulina | 12 | 0.125 (−0.315, 0.564) | 0.579 | 98.5 | |
| Chlorella | 7 | −0.043 (−0.129, 0.042) | 0.321 | 46.8 | |
| Others | 5 | −0.084 (−0.179, 0.011) | 0.082 | 26.3 | |
| Health condition | |||||
| Health | 7 | −0.132 (−0.224, −0.039) | 0.005 * | 76.6 | |
| Type 2 diabetes | 5 | 0.036 (−0.670, 0.743) | 0.919 | 98.9 | |
| Obesity | 8 | 0.158 (−0.401, 0.716) | 0.581 | 98.9 | |
| Other unhealth conditions | 4 | 0.119 (0.001, 0.238) | 0.048 * | 0.0 | |
| Area | |||||
| East Asia | 14 | 0.095 (−0.184, 0.373) | 0.701 | 98.5 | |
| Non−Asia | 2 | −0.055 (−0.636, 0.526) | 0.853 | 79.5 | |
| Southwest Asia | 8 | 0.042 (−0.059, 0.144) | 0.413 | 0.0 | |
| TG(mmol/L) | Intervention duration | ||||
| <10 weeks | 7 | 0.186 (−0.345, 0.717) | 0.493 | 57.6 | |
| >10 weeks | 15 | −0.112 (−0.551, 0.326) | 0.616 | 82.3 | |
| Sample size | |||||
| <40 | 11 | −0.110 (−1.123, 0.902) | 0.831 | 86.9 | |
| ≥40 | 11 | 0.116 (−0.058, 0.289) | 0.190 | 22.5 | |
| Intervention species | |||||
| Spirulina | 11 | −0.266 (−0.940, 0.408) | 0.439 | 87.6 | |
| Chlorella | 7 | 0.151 (−0.155, 0.456) | 0.335 | 46.4 | |
| Others | 4 | 0.030 (−0.549, 0.609) | 0.919 | 0.0 | |
| Health condition | |||||
| Health | 8 | 0.463 (0.017, 0.909) | 0.042 * | 73.1 | |
| Type 2 diabetes | 5 | −0.472 (−1.451, 0.507) | 0.345 | 87.9 | |
| Obesity | 3 | 0.091 (−0.782, 0.965) | 0.838 | 0.0 | |
| Other unhealth conditions | 6 | −0.558 (−1.412, 0.297) | 0.201 | 74.7 | |
| Area | |||||
| East Asia | 11 | 0.183 (−0.366, 0.751) | 0.514 | 86.0 | |
| Non−Asia | 2 | −0.180 (−0.679, 0.318) | 0.478 | 0.0 | |
| Southwest Asia | 9 | −0.294 (−0.848, 0.259) | 0.297 | 62.6 | |
| TC(mmol/L) | Intervention duration | ||||
| <10 weeks | 9 | −0.128 (−0.383, 0.127) | 0.325 | 79.6 | |
| >10 weeks | 16 | −0.646 (−0.991, −0.300) | 0.000 * | 88.0 | |
| Sample size | |||||
| <40 | 11 | −0.242 (−0.513, 0.030) | 0.082 | 83.5 | |
| ≥40 | 14 | −0.700 (−1.101, −0.299) | 0.001 * | 90.0 | |
| Intervention species | |||||
| Spirulina | 13 | −0.803 (−1.223, −0.383) | 0.000 * | 90.1 | |
| Chlorella | 6 | −0.016 (−0.310, 0.278) | 0.914 | 79.0 | |
| Others | 6 | −0.242 (−0.518, 0.034) | 0.085 | 48.6 | |
| Health condition | |||||
| Health | 5 | −0.692 (−1.269, −0.115) | 0.019 * | 94.3 | |
| Type 2 diabetes | 5 | −0.072 (−0.250, 0.107) | 0.432 | 0.0 | |
| Obesity | 9 | −0.346 (−0.553, −0.140) | 0.001 * | 59.2 | |
| Other unhealth conditions | 6 | −0.810 (−2.137, 0.516) | 0.231 | 94.0 | |
| Area | |||||
| East Asia | 13 | −0.475 (−0.723, −0.226) | 0.000 * | 88.0 | |
| Non−Asia | 2 | −0.200 (−0.507, 0.107) | 0.202 | 0.0 | |
| Southwest Asia | 10 | −0.582 (−1.276, 0.113) | 0.101 | 89.6 |
| Outcomes | Begg’s Rank Correlation Test | Egger’s Linear Regression Test | ||||
|---|---|---|---|---|---|---|
| Z Value | p-Value | Intercept (95% CI) | t | df | p-Value | |
| FPG | 0.29 | 0.773 | −0.04 (−1.51, 1.44) | −0.05 | 16 | 0.959 |
| 2hPBG | 1.13 | 0.260 | 3.77 (−0.71, 8.24) | 2.34 | 5 | 0.080 |
| HOMA−IR | 0.24 | 0.806 | 0.40 (−1.26, 2.06) | 0.76 | 4 | 0.503 |
| Insulin | 0.73 | 0.466 | −1.92 (−4.02, 0.19) | −2.16 | 8 | 0.068 |
| HbA1c | 0.89 | 0.371 | 1.34 (−0.86, 3.54) | 1.41 | 9 | 0.197 |
| HDL−C | 0.21 | 0.833 | −0.88 (−2.84, 1.07) | −0.94 | 22 | 0.360 |
| LDL−C | 0.72 | 0.472 | 0.66 (−3.69, 5.02) | 0.31 | 24 | 0.756 |
| TG | 0.11 | 0.910 | −0.26 (−1.81, 1.28) | −0.36 | 22 | 0.726 |
| TC | 0.61 | 0.544 | −0.89 (−2.65, 0.87) | −1.04 | 24 | 0.307 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, K.-x.; Gao, T.-l.; Xu, R.; Cai, J.; Zhang, H.-q.; Sun, Y.-y.; Zhong, F.; Ma, A.-g. Quantifying the Effect of Supplementation with Algae and Its Extracts on Glycolipid Metabolism: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 12, 1712. https://doi.org/10.3390/nu12061712
Ding K-x, Gao T-l, Xu R, Cai J, Zhang H-q, Sun Y-y, Zhong F, Ma A-g. Quantifying the Effect of Supplementation with Algae and Its Extracts on Glycolipid Metabolism: A Meta-Analysis of Randomized Controlled Trials. Nutrients. 2020; 12(6):1712. https://doi.org/10.3390/nu12061712
Chicago/Turabian StyleDing, Kun-xiang, Tian-lin Gao, Rui Xu, Jing Cai, Hua-qi Zhang, Yong-ye Sun, Feng Zhong, and Ai-guo Ma. 2020. "Quantifying the Effect of Supplementation with Algae and Its Extracts on Glycolipid Metabolism: A Meta-Analysis of Randomized Controlled Trials" Nutrients 12, no. 6: 1712. https://doi.org/10.3390/nu12061712